
The Next Big Thing?
Microdermals and Surface Anchors
Microdermals — or “surface anchors”, or simply “anchors” — are a design of body jewelry that allows for a “single point” piercing. That is, a piercing that has only one visible end or bead. So for example, it allows one to place a single gemstone in a third eye position, and because of its design, no invasive procedure is required to implant it — it does not have the complexity of implantation of a transdermal implant (although it may have some of the complexity of removal). In addition, its versatile nature makes it an excellent tool for unusual formations of piercings as of course any number may be placed.

“THIRD EYE” MICRODERMAL PLACEMENTS;
LEFT: IAM:PUREANGEL BY BRIAN DECKER, RIGHT: BY JOHN DURANTE (IAM:JAWN D)
Since their introduction as a prototype by Custom Steel at APP 2006, microdermals have been explosively popular with most users becoming convinced that these could be the next big thing in piercing, and arguably the first “new” idea in some time. That said, the technology has been around in other forms since the mid-nineties — Steve Haworth went through several designs of transdermal implant which heavily influenced their design, as did the single point pocketings first promoted by Jon Cobb, as well as dermal anchors (gallery) and other DIY-anchor techniques. In addition, surface bars, and especially the later punch-and-taper (or punch-and-elevate) procedures, involved related techniques and healing, which influenced the design and development of microdermals.
Since they’ve been growing in popularity now for a solid six months, I feel somewhat tardy waiting this long to talk on the public record with artists performing microdermals, but the good side of that is that now enough time has passed that people can reflect on healing and the ongoing development of microdermals and related procedures. Let me begin by introducing the people I talked to (in no particular order), a small cross-section of the piercers and jewellers performing this procedure and making these devices. Ask around to find more!
BASIC MICRODERMAL DESIGN — A SMALL BONE PLATE WITH HOLES FOR TISSUE INGROWTH, AND A THREADED POST FOR THE ATTACHMENT OF DECORATIVE ENDS.
Oh, and just so there’s no confusion — these interviews were conducted separately, so don’t read anything into any implied interactions between them!
 |
Bryan Thomas
Mojo Studios, Peoria, IL
iam:cellfire |
Didier Suarez
Enigma Professional Piercing, San Diego, CA
iam:DidierS |
 |
 |
John Joyce
Scarab Body Arts, Syracuse, NY
iam:j_scarab |
Steve
“Travelling”
iam:micro-wave |
 |
 |
James “Wizzer” Wisniewski
Hollywood, CA
iam:Wizzer |
Brian Decker
Pure Body Arts, Brooklyn, NY
iam:xPUREx |
 |
 |
Pat Pruitt
Custom Steel Body Jewelry
iam:[email protected] |
JLo (John Lopez)
Slave to the Needle, Seattle, WA
iam:JLo |
 |
 |
IME
Integrity Body Jewelry
iam:IME |
Shannon Larratt
BME
iam:glider |
 |
| |
How would you describe what a microdermal is? |
|
BRIAN |
The idea is to give the aesthetic look of a transdermal implant but with the simplicity and safety of a piercing. |
DIDIER |
A microdermal is a single-point surface piercing with a threaded changeable end. |
JLO |
I don’t call them “microdermals”. I called them single-point-piercings until Industrial Strength introduced their surface anchors — I like that name.
Eight or nine years ago I tried something like them, using 14g fishtail labret jewelry — which was a horrible disaster. Maybe a year and a half ago I saw somebody on IAM was using nostril screws and having some success. I tried some myself with not so good results — the results were 50/50 at best.
|
PAT |
Sorry to say, but bending up nostril screws to be used as anchors is super-ultra ghetto if you ask me, and being a part of this industry, I hated to see something misused like that. There is enough talent in this industry to have stuff like this professionally made — hence the new microdermal. |
JLO |
A fellow piercer at Slave to the Needle, David, and I started drawing pictures and debating design ideas to create something similar to the transdermals in David’s scalp but much smaller. We wanted something that required standard piercing tools only — no surgical tools. Something any seasoned professional piercer should be able to do. Strangely enough, I got the call from Pat at Custom Steel that very week. |

MICRODERMAL JEWELRY; LEFT: IME’S PROTOTYPES, RIGHT: IS SURFACE ANCHORS (ALMOST IDENTICAL TO CUSTOM STEEL MICRODERMALS), INSET: ANCHOR BY BRIAN DECKER
PAT |
I started playing around with the idea about a year ago after seeing the dermal anchors being installed. I thought that piece of jewelry really sucked ass for that particular application (it was more or less a bent up nostril screw). I gave it a lot of thought before sending a CAD drawing to John Lopez to check out (because of his experience with dermal anchoring) and Phish (because of his experience with implants) to get some initial feedback in February of this year. |
JOHN |
When I first saw the dermal anchors, I knew they were a bad idea… but I thought it had potential. A few practitioners started doing variations of the “dermal anchor” with bent nostril screws, but I still wasn’t sold. The first true microdermals I heard of were Pat from Custom Steel’s pieces at APP 2006, machined out of solid titanium. This new design made far more sense to me. It had borrowed from transdermal design. It had little holes in the base that the skin could anchor in, but was small enough that it could be inserted easily, without the need for a scalpel, sutures, or elevators. JD from Industrial Strength had designed a very similar version, and offered me samples — I was amazed at how small they were. It was mind blowing! They came with a healing nub, very similar to transdermals, but any 14 gauge bead could screw onto them. |
JLO |
A few months after I talked to Pat, I was invited to visit JD at Industrial Strength. He flew me out to California and took me on a tour of his manufacturing facilities and showed me his version of the very same idea. He was calling them “surface anchors”. This is a great name because it doesn’t sound quite so “medical”. JD gave me a bunch to try out and I instantly knew these things were going to get big… and I still think they will. |
PAT |
Noah Babcock from Evolution Body Piercing in Albuquerque, who I would consider a master at surface piercing, guided me through potential installation procedures with such a small device, staying in the realm of common piercing instruments. The goal was to produce an implantable fixture, that could have interchangeable ends, that could be installed with no medical tools, but only common tools found in any shop — so no scalpels or punches… just piercing needles and tapers. The first prototype run debuted at APP 2006 and went out to a handful of clients on the down-low… they’re healing very nicely with no issues. |
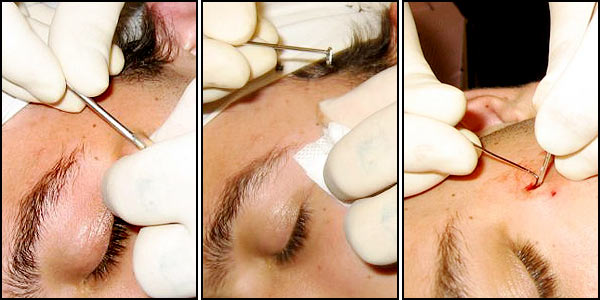
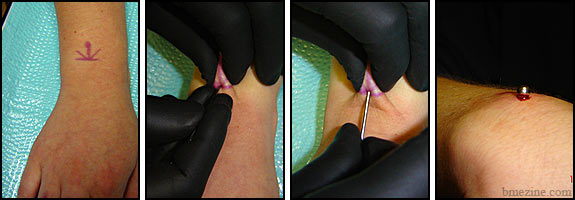
TYPICAL MICRODERMAL INSERTION — 1. ENTRY/EXIT POINT IS MADE USING A NEEDLE OR DERMAL PUNCH; 2. MICRODERMAL JEWELRY IS INSERTED INTO THIS HOLE AND USED TO ELEVATE A POCKET AS NEEDED; 3. JEWELERY IS SETTLED INTO PLACE.
BRYAN |
After I saw pictures on Pat’s page I thought they were neat, and I tried one on myself. |
STEVE |
I started hearing about them this summer when several of my friends began talking about them and I got messages from manufacturers advertising them. At first I had a lot of fears and apprehensions regarding them, but my friends kept telling me of their successes with them. After I kept hearing positive things about microdermals, I did my first in August on a good friend of mine, a ‘third eye’ placement. |
BRIAN |
I actually began doing something similar about a year ago, but with a different design of jewelry that spiralled into the entrance. The piece had a central base point rather than the more common design which anchors itself mostly only on one side of the base. The idea, for me, came about quite a while ago, when I was searching for a more cost effective way of making transdermal implant pieces. The first one I did was, and still is, in the wrist of iam:Peck. |
WIZZER |
I also started working with the microdermal concept using hand-bent jewelry. I started using the microdermals produced by Industrial Strength a few months back and I am now working with prototypes made by IME of Integrity Body Jewelry. Overall, I’ve done over a hundred of these, every one being successful in both procedure and healing! |
IME |
I did a few with nostril screws in 1999, but ever since Pat from Custom Steel came out with them at APP this year I have had a ton of people asking me to come up with a design of my own. I have been prototyping them for a few months in my spare time and started doing them on friends, to make sure the design is stable. |
MICRODERMAL PROCEDURE BY KEITH ROMAN (KYKLOP TATTOO, PITTSBURGH PA)
| |
Does anyone specific deserve credit for developing the microdermal? |
|
PAT |
I think I can solidly hold claim to the latest design of the microdermal, hell, I even coined the term “microdermal”. |
STEVE |
I agree. |
BRIAN |
Yes, the pieces I make are based on Pat’s design. They’re much easier to insert than my older idea. |
JLO |
I think Pat and JD both were working on them at the same time, and IME at Integrity has come up with a variation that just might provide some specific solutions. I know that many piercers have been working on the idea for well over ten years. |
WIZZER |
I’m sure the idea of single-point microdermals or dermal anchors have been used by many people in shops never heard of, so I can’t give credit to anyone specific. |
DIDIER |
It seems the design was no more than a small bone plate with a 3/32” barbell post placed to one side. After the first prototype was made and we all started testing the prototypes, we’ve had three or four changes in the anchor since the beginning. |
| |
Why use a microdermal instead of a surface piercing, a transdermal, or even an older method like a dermal anchor (or single-point pocketing)? |
|
BRYAN |
Movement barely affects microdermals. Time will prove that statement, but I’ve seen microdermals be successful in places where surface bars would fail. The really great thing is the procedure — because they’re so tiny, there’s no need for an incision or sutures — it’s just a 14 gauge needle! |
JLO |
I’m not sure what the difference is between “microdermals” and “dermal anchors”. I’ll refer to the 14ga single-point jewelry as anchors from this point on. The main advantage of anchors over transdermal implants is they’re frickin’ tiny! The fact that a needle and a pair of hemostats are the only tools needed rocks! Anchors can be used to create odd number patterns that weren’t possible with surface piercings — they can be placed nearly anywhere you want. And of course, we can now “bedazzel” tattoos! Weeee! |
JOHN |
Microdermals should replace older methods like dermal anchors all together. I think there are some instances where a microdermal can replace a transdermal, but not in every instance. |
BRIAN |
A microdermal seems to be more stable in areas of movement than a surface bar is because of the reduce pressures, but I believe transdermal implants are a more permanent, sturdy, and stable procedure, mainly due to their size and centred bases, and less likely to tear or reject. |
JOHN |
I’m far more comfortable offering the microdermal to my clients, since it can be done without the surgical aspects that a transdermal requires, making it safer for myself and the client. A microdermal far easier to remove, with less scarring involved. |
PAT |
It’s a transdermal on a much smaller scale, but in comparison to the dermal anchor they’re one and the same — just a different base design with the interchangeability of decorative ends.
I’m sure there will still be a place for surface piercings on some individuals, but with the microdermal, it opens up the door for precision placement, less trauma, faster healing time, and almost zero migration issues. Compare that with the issues involved with surface piercings! I do believe this will replace surface piercings.
|
WIZZER |
These microdermals will be giving surface piercings a good run for their money, but won’t replace them. It definitely opens many new placement opportunities, and healing times are drastically shorter, and longevity better, than with surface work from what I’ve seen. I’ve also been using these in replacement of standard navel piercings on clients who have a “true” or “outie” navels! Another use for these are lip or labret piercings, making the concern about tooth damage and gum erosion a thing of the past. |
DIDIER |
I’ve also done them for labrets, cheeks, and other oral piercings for prevention of gum recession, and they work great. |
WIZZER |
While working with these for the past six months, their popularity has been increasing rapidly. People who have no interest in piercing whatsoever seem to love the idea of having some “bling” off to the corner of one eye. A new door has definitely been opened. |
DIDIER |
Because microdermals are independent, it allows the skin to move, pull, and stretch freely. You still have to pay attention to the bodies folds and creases, but the free movement allows the body to heal with less scarring. Coming from the perspective of a service that could be offered to clients in a regular walk-in studio, I think it’s a less invasive modification than transdermals, and can offer some of the same desired looks. |
JOHN |
I kind of rate these new microdermals right along with surface piercings, but, to be honest, these microdermals in many instances are actually easier to do that some surface piercings. That said, most piercers don’t fully understand how surface piercings work, and most aren’t using the correct jewelry or placing them properly. I’m sure that many piercers won’t get how these new microdermals work. I only wish that practitioners that didn’t understand would ask someone who does, instead of trying to figure it out on their own by using clients as guinea pigs. |

“FRANKENSTEIN” MICRODERMALS BY WIZZER
| |
Do you consider it an implant or a piercing? |
|
BRYAN |
It’s easier to get done than a “normal” implant, since it doesn’t require minor surgery, but you are still putting something under the skin that may require some effort to get out. So it’s still an implant. |
PAT |
You’re using piercing-only techniques to install an implant — so it’s a hybrid. |
BRIAN |
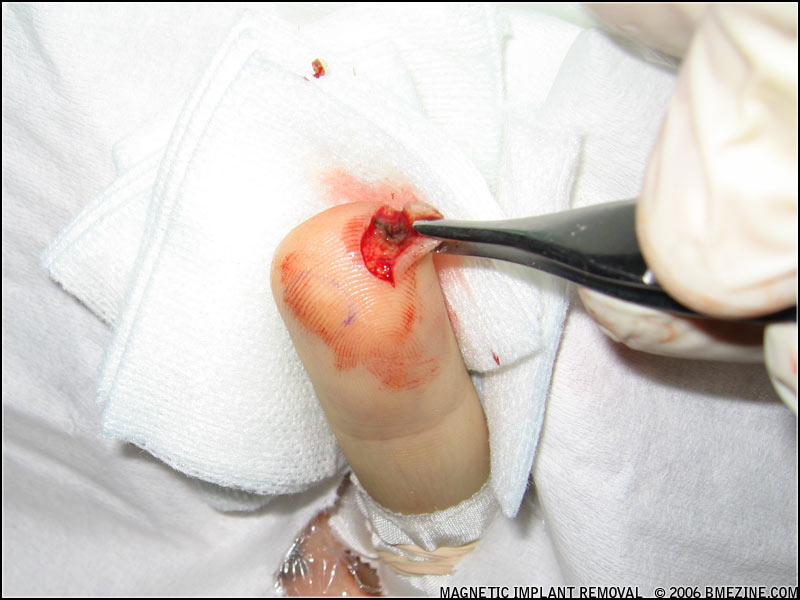
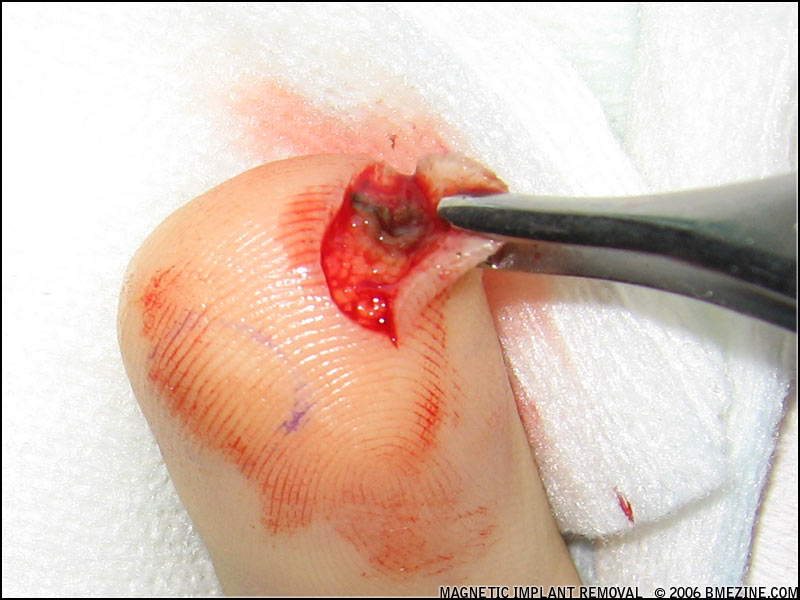
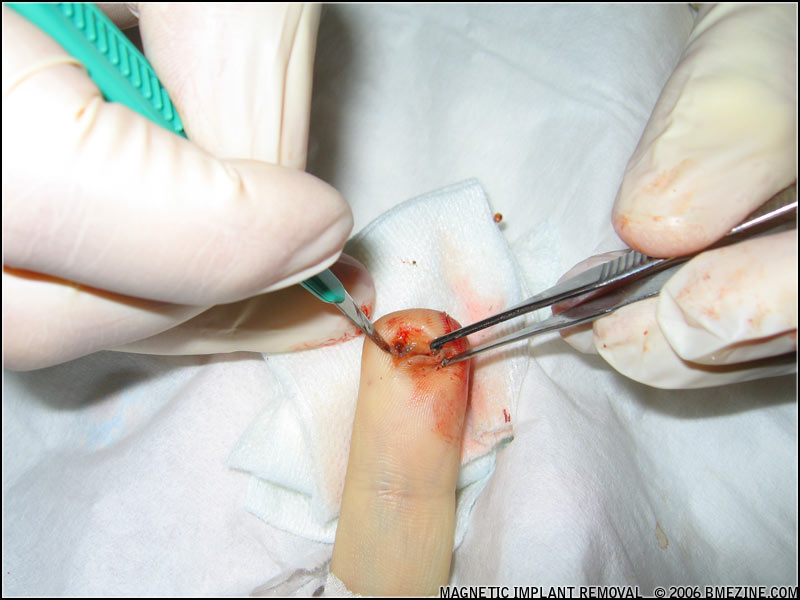
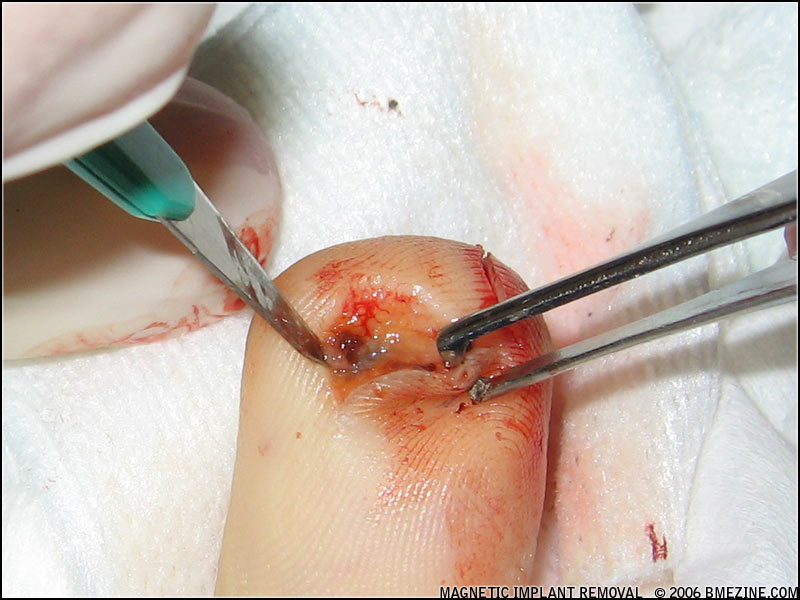
Once healed into place, for removal the microdermal will need to be cut out. It still won’t be as difficult to remove as a transdermal, but the client most likely will have a very difficult time trying to remove them alone. |
DIDIER |
The tissue through the holes isn’t as strong as most would believe. |
JLO |
I think it’s a piercing. Definitely. In fact, I charge the same for an anchor as I do for a nostril piercing! |
STEVE |
It lies in the middle. Being that they can be inserted via traditional piercing techniques, they’re very accessible to artists who feel comfortable with doing piercings but not doing implants. |
JOHN |
It’s definitely closer to a piercing. One thing I love about these so much is they can be done with a piercing needle. In areas with strict regulations, where implants, or the use of scalpels, are prohibited, microdermals should be fine since the only thing you need to install them is a piercing needle. |
DIDIER |
I think it’s a piercing all the way.The anchor is like a one sided flat surface bar. |
IME |
It’s closer to a piercing in my opinion. |
| |
Do you mind describing the procedure you use to install them? |
|
JLO |
I pierce the skin using a 12 gauge needle, in a similar way to how I do surface piercings, but the needle only goes in the depth of the bevel and then comes right back out. Then I use a modified pair of hemostats to hold the anchor (with a mini disk screwed in), and do the insertion. |
DIDIER |
I’ve done over a hundred with needles. I used a 10 gauge at first, which I suggest for beginners, but I’m going between 12 gauge and 11 gauge right now. Some parts of the body require a small needle because of the thickness of the tissue. |
BRIAN |
I install microdermal pieces into pockets, fully in the subcutaneous layer of skin, through a 1.5mm punched hole. After punching out the entrance point, I use a small 2mm wide flattened elevating tool to make a pocket for the main, longer part of the microdermal piece. I turn the tool around and make a second, smaller pocket for the “heel” of the piece. With the jewelry threaded onto a 2mm taper, I insert the long section of the base into the larger pocket and push in and downward until the punched hole is stretched enough for the “heel” to snap down into place. Last, I unscrew the taper and thread on the chosen end piece to the base. Generally, the pieces I use have 3mm tall lifts, and are about 5 or 6mm long. |
STEVE |
My procedure was taught to me by Leo Ziebol of 5 Point Studios (iam:5point). To make the channel, I use a 1.5mm biopsy punch with a small silicon o-ring on it to control depth. I attach the microdermal to a threaded taper and slide the ‘foot’ of it under the tissue, using the ‘foot’ to elevate the skin and find a good area for the base to lie. The ones I’ve used have a smaller end on the other side of the base, and I massage and manipulate the skin to place this end at the same depth as the other side of the base. After making sure it is sitting well, I remove the taper and attach the end [bead] on top, lightly massaging the tissue afterwards to ensure it all sits properly. |
IME |
I use a needle. The microdermals that I have been making match the crescent shape a needle makes. |
JOHN |
I tried a couple with a 10 gauge needle. Everything went fine, but I found I like a 1.5mm dermal punch better since it is very similar to how I do surface piercings (using the “punch-and-taper method”). What I do first is clean the area with Technicare, and then mark where it is going to be. I pinch up the skin where the mark is, and insert the 1.5mm dermal punch straight down into the skin. Once that hole is there, there is no need to use a taper to elevate the skin like you would with a surface piercing — you can just use the leg of the microdermal to separate the tissue for itself. Using a pair of hemostats, I hold the microdermal by the healing nub, and place the long leg of the piece into the hole, lean it back, and pop the short leg into place. The whole procedure is very fast; faster than a surface piercing. |
WIZZER |
I use a 1.5mm dermal punch to create the initial hole for the base to be inserted through. I found that I get a better, more flush seating with the jewelry under the tissue using this method, as opposed to using a larger gauge needle. For easier insertion and better control, I use threaded tapers as a handle which screw into the base. Then it’s a simple pinch and push to seat the jewelry in the hole. The threaded taper then unscrews, and the desired threaded end is put in place. I only finger tighten my ends to prevent the base from rotating under the tissue when the ends are changed. |

LEFT: BAT EYES TATTOO DECORATION BY KEYLAN LEVINE (IAM:XKEYX), RIGHT: TWO WEEK OLD CLEAVAGE ANCHOR BY DIDIER
| |
How is the procedure from the client’s point of view? Is it something people want anaesthetics for, or is it no more traumatic than a piercing? |
|
BRYAN |
It’s on the same level as a surface piercing. Anaesthetics aren’t really necessary for doing them. |
JLO |
In certain parts of the body it can hurt quite a bit, but in other areas it’s just stupid-easy. Thicker skin such as the lower back creates a much more intense sensation, and thinner skin with a lot of elasticity such as the forehead or throat is easier. |
DIDIER |
I think the procedure is the easier than most piercings, if done right. Sometimes it can take a minute to make sure the anchor is sitting flat, but better then than later. |
BRIAN |
Anaesthetics are never necessary for installing microdermal pieces. The entrance punching is usually the most painful part of the procedure, and is very minimal. It takes less time to put in than a punch and elevated surface bar, and is even less intense than that. Installing a microdermal piece usually takes under a minute. |
STEVE |
The friends I’ve installed them on so far say it is a very light procedure — they have been quick, clean, and easy. |
JOHN |
Anaesthetics aren’t necessary at all. As I said earlier, it’s basically the same technique I’ve been using for surface piercings. The clients that I have done the procedure on have all said it was one of the easier procedures they have been through. |
| |
Have you done many? |
|
BRYAN |
Just the one on me. |
JLO |
Well over forty now I’m sure. |
DIDIER |
I’ve had the advantage of working with Industrial Strength from the first prototype. So, like I said before, I’ve done over a hundred, and I have a few projects that required multiple anchors. |
STEVE |
I have only done four — a ‘third eye’, and a set of three on a sternum. So far the third eye has healed without any incident, and the sternums, which at first were bothered by the person’s activities combined with the ends, are now doing well. |
JOHN |
At this point I’ve done a bit over a dozen of them, and have a few more lined up. All the ones I’ve done so far are still in, and have healed, or are healing fine. I’ve only removed one so far. That wasn’t due to any healing or irritation problems — the person needed it removed for her job. |
BRIAN |
I’ve done quite a few now, yes. They are growing more known and are a more stable option for a lot of areas than surface bars — but I only suggest them for clients who know they will not be as easy to remove as a surface bar. |
| |
How have they been healing, and what is your recommended aftercare? |
|
BRYAN |
Mine is about a month and a half old, and healing has been very, very easy. I’ve gotten a little crust out of it and that’s about it. I used the LITFA method along with H2Ocean five or six times — I’m really lazy when it comes to aftercare. So far, things are going well, and it’s been one of the easiest things to heal ever… much easier than a surface piercing. |
JLO |
Healing seems to be fairly consistent from person to person, and body part to body part. I’ve noticed that it takes longer than I suspected — about three months. At about six to eight weeks they often become quite “juicy” and a bit angry. Then within a couple weeks they settle back down and finish healing. I only suggest warm, moist compresses when they itch, swell, or otherwise need attention. Otherwise I suggest completely ignoring them. |
STEVE |
The aftercare I’ve suggested has been the same I suggest for a standard piercing — keeping the piece safe, free from stress, free from irritants, clean, dry, and just generally giving your body a good environment to heal in. The healing processes have been uneventful and comfortable for the wearers. |
BRIAN |
Thus far I don’t know of anyone that’s had problems with my microdermal pieces. Even in the center of iam:amnesiac’s lip, it appeared healed in only a week or so. The only real problem I had with one was Steve Truitt’s nape — the piece I was using from Industrial Strength only had a 2mm rise, and the tissue in his nape was much thicker. We only had a disk end piece at the time, which made for a much too tight fit.
The aftercare that I suggest is no different than with a surface bar — dry heat compresses and sterile saline washes is all I have my clients do for healing.
|
DIDIER |
I’d have to say 98% success in healed healthy anchors. I’m suggesting cool saline pads for the first day or two, and after that I’m having my clients do warm compresses with saline. I’m asking that they not change the end for two or three months. |
| |
Wow, 98%? You think you’ll really get 98% success in the long run? |
|
DIDIER |
Time will tell. I think certain placements will do better long term. |
IME |
So far complete success. I recommend taping it for the first few days, keeping it dry, and leaving it alone — but I am a “leave it alone” kind of guy. |
JOHN |
Healing success so far has been great, and no problems have been reported. I’ve basically been telling people to leave them alone — keep all soaps, lotions, and everything else away from them. I do like the Simple Care Spray from Body Art Pro. The client can just spray it on once or twice a day — that way they feel like they are cleaning it, so I don’t have to worry about them trying something else that may irritate it! |
WIZZER |
My suggested aftercare for these is the same as any piercing I do: an inverted cup of warm saline solution, held to the piercing for five minutes, twice daily, followed by the area either air drying or being pat dried with a disposable, lint-free paper towel product or gauze. I usually dress the microdermals with a Tegaderm bandage after the procedure and provide two extra pieces for the clients to apply before sleep for the following two nights. |

PROCEDURE ON IAM:CURSETHISMETALBODY BY IAM:MUTE-ONE
| |
How robust are they? Do they hold up well to sleeping on them, impacts, bead changes, and stuff like that? |
|
STEVE |
Their relatively small size compared to transdermals, and some surface piercings, caused me to worry initially about how they would hold up to impacts and stress. So far, the wearers haven’t encountered any large amounts of stress on them, and I haven’t heard of it being a problem from my friends who install them. The bead changes I’ve done have been very simple and caused no irritation. |
BRYAN |
I’ve only snagged mine on clothes a few times, and it’s still in there! You need to be really gentle when changing the ends on them — it feels like you are going to pull it out. I’ve seen a few pictures of people who pulled them out while changing the ends on them. |
JLO |
Obviously, the longer they are healed, the more they can handle. After the body really grabs them they are quite resilient, but since they are so small, a good snag has the potential to rip them right out. One of my customers had to change her bedding completely because of the lace that constantly found a way to wrap around the disk!
The ones I have on my temples get banged and pulled daily by my one year old daughter. I’ve had them for about five months and I don’t even pay attention anymore. No pain, and no problems at all.
|
BRIAN |
I don’t think microdermals, with the most recent jewelry designs, have been around long enough to know. I’ve done end changes with no problems, but as far as impact resistance, I still think a transdermal implant will be more stable — but a surface bar less. |
JOHN |
For how small the are, they are very robust. I’ve done a couple on wrists, which are notorious for giving surface piercings problems… yet these microdermals seem to be holding up fine. The initial healing nub can get knocked around a bit, especially while sleeping, but it doesn’t seem to cause long term damage like it does for many piercings. |

LEFT: LOWER NAVEL BY BRIAN DECKER, RIGHT: CLEAVAGE BY WIZZER
| |
How did you learn to do them? |
|
DIDIER |
I started with myself, and other piercers and counter staff. After a few months I contacted most of my regular clients and offered the service in exchange for information on the anchors. |
STEVE |
I took the time to think about the procedure, and talked to a couple friends who had done them before attempting one. Leo Ziebol told me his procedure and I adopted it. |
JLO |
I have great guinea pigs working the counter at Slave to the Needle — these people let me do anything to them if it’s free. LOL. |
JOHN |
I talked with a few practitioners that had already installed them. I found out what methods they were using, and what drawbacks they had come across from them. I had a lengthy talk with Tom Brazda about them at APP 2006, before I even knew they would be so readily available. After talking to so many practitioners that I respect and getting their input, and since I had been using the punch and taper method for so long, I was confident in my ability installing these pieces. |
BRYAN |
Just common sense and asking other piercers some questions. |
BRIAN |
Yes, nothing more than common sense and second nature, I think. I’ve been doing implants and punch and elevate surface style piercing long enough that it just made complete sense right away. |
| |
Are any skills on top of “good piercer” required to install a microdermal? |
|
DIDIER |
I think most skills can be applied from piercing. In my experience, the motion of the needle is like a “dip” when doing a surface piercing. The finger position is a little different, but varies depending on how difficult it is to pinch the tissue. |
BRIAN |
With the method of insertion I use, a good understanding of measuring and feeling for tissue depth is important. Otherwise the piece may not sit fully in the subcutaneous layer, and may pull an end piece down under the skin if placed too deeply, or facilitate rejection if done too shallowly. Anyone who understands punch and elevate surface technique should have no problem with these. |
JLO |
Being able to read the grain of the skin and visualizing the jewelry in the tissue helps a lot. |
STEVE |
I think any artist that devotes an appropriate amount time and effort into researching microdermals is capable of doing them. This means someone who knows how to install them with minimal trauma, what qualifies as appropriate placement and use, a good base of knowledge and experience regarding aftercare, a sense of preparation in case something goes wrong during the procedure or during healing, knowledge on their removal, knowledge on sterile procedures and cross-contamination, care for the wearer, and good intentions. |
JOHN |
Being a good piercer is a start. Having some experience in elevating the skin for surface piercings would help — that can be from punch and elevate or from pierce and elevate methods. Knowing how the skin elevates and separates makes it easier to grasp installing these. Confidence in yourself is important, but without arrogance — knowing when you’re not ready, and having the morals, ethics, and responsibility to admit it is important, and unfortunately that is something a lot of people in our industry don’t seem to understand. |
IME |
I found it to be really simple. |
PAT |
Here’s the scary part — with the finesse of the design, you don’t even have to be a good piercer to install these! |

LEFT: TWO WEEKS OLD BY KEYLAN LEVINE (IAM:XKEYX), RIGHT: BY JOHN JOYCE
| |
What advice would you have to other piercers who would like to start doing this procedure? |
|
BRYAN |
After some research, practise on yourself first — or at least on a really trusting friend. |
PAT |
Like with everything watch, learn, and do research here on BME… or practise on friends and family. These are so simple to install — it’s pretty amazing. But I’m not gonna be offering the jewelry to just anyone. Due to the number of hacks out there that are willing to do anything to make a buck, I’m keeping my clientele to a very short list. |
JLO |
They’re easy enough. All you need to do is do them in your mind first. The not-so-obvious problems seem to show themselves that way. Then be ready to improvise when you actually attempt them. If they don’t sit right, don’t be afraid to remove them the next day and massage the skin and immediately reinsert them. Play with them a little and you’ll find a technique that works for you. Sky Renfro (from propiercing.com) is working on setting up a class too! That’ll be so awesome to experience other piercers’ techniques as well! |
DIDIER |
I would suggest video taping what you are doing, and taking your time. Do a dozen in four months — not in four days. Watch your video and learn from your successes, as well as your failures. And if you take your time, your success rate will be higher. |
BRIAN |
Even if piercers are seasoned and have no problems with getting the pieces into the skin, they should limit them to clients who understand they will be difficult, and most likely painful, to remove. |
STEVE |
There are lots of very talented and friendly artists doing these procedures — talk to them and make sure you feel comfortable with every step of the procedure before attempting it. Understand everything from the purchasing of the jewelry, proper sterilization and installation, and long-term aftercare, and its possible removal. |
JOHN |
Ask for help. Ask someone you respect that you know has done these — find out how they did it. If you live near someone doing them, ask to watch them do one. Hell, ask them to do one on you! Then you get a firsthand experience of how they are done, and how they heal. This is all knowledge you can share with your clients. |
PAT |
The long-term degree of adherence of the microdermal to the underlying tissue is still unknown… Noah has the longest running microdermal of mine to date at six months. I have a feeling with the microdermal being implant grade titanium, these may have to be cut out and away from the tissue that bonds to the titanium. People should consider them permanent as long as healing and removal information on fully healed microdermals — one year plus — remains unknown. |
IME |
Look around as see what other people are doing. This is a newer item and a lot of people are doing different things — try and check them all out. |
| |
What advice would you have to clients looking to have one of these done that isn’t already a friend or regular of a piercer doing them? |
|
DIDIER |
If your regular piercer can’t do the procedure, ask for a referral. Do your homework — like for any other piercing. |
STEVE |
Make sure you feel safe and informed on the procedure. Also, these particular pieces are new inventions in our industry and we are still learning about them — keep that in mind. |
JOHN |
While they seem to be working our really well, their success can’t be guaranteed. Along the same lines though, no piercing can really be guaranteed… |
JLO |
Until anchors have been around for four or five years I think we must think of them as being in a trial phase. |
BRYAN |
I probably wouldn’t do one on a client — maybe on another piercer who knew the risks and such, but these things are still too new for me to be doing them on customers. Besides, removal will require some cuts… |
BRIAN |
Clients need to know these pieces are borderline permanent, with respect to ease of removal. |
JOHN |
Research it, and research the artist doing it — research everything. Make sure you want it and consider it a permanent choice. I know these aren’t as “permanent” as transdermals, but they are more permanent than your standard piercing. Even if the microdermal isn’t permanent, any scars left behind from it (or any piercing) can be. |

LEFT: TEMPLE BY KEYLAN LEVINE (IAM:XKEYX), RIGHT: SELF DONE BY BRYAN
| |
Does the design of the microdermal still need refinement, or do you consider the current design “mature”? |
|
JOHN |
It’s still new and in its testing phase as far as I’m concerned. |
PAT |
My original design had a lot of time and thought into it. Aside from the variables (number of holes and post length) there isn’t much room to improve upon. That said, I am working on some finer points to the microdermal that I’ll discuss and debut at a later date. |
DIDIER |
I can’t see what I would do different with the design. Anything to make the anchor less likely to reject or pull out would make it more difficult to insert or remove — I’ve been told that Industrial Strength is also working on different variations of the anchors. |
STEVE |
I’ve only had experience with one model of microdermal, and I thought it was very appropriate for its usage — but I won’t be surprised if we see better models out as the popularity of this jewelry rises. |
BRIAN |
For ease of insertion, I can’t think of a shape that would work better right now, but perhaps a design that doesn’t have permanent anchoring of skin through the jewelry would be a good idea. If the main section of the base looked more like a tuning fork with two “legs” rather than holes, the piece would still be able to anchor as scar tissue would build up in the gap, but removal would be much simpler. |
WIZZER |
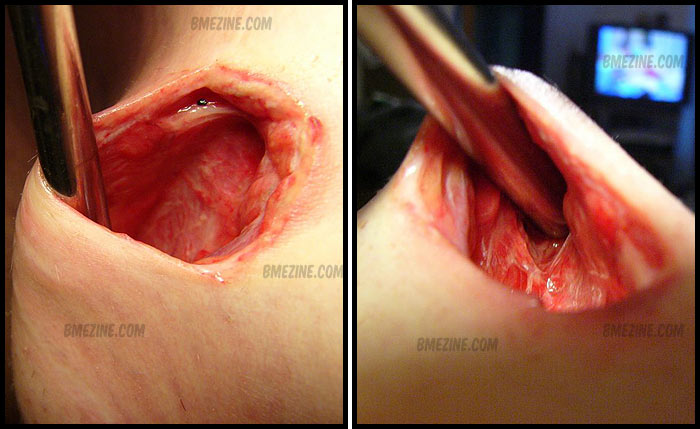
I feel the Industrial Strength microdermals work really well — the only issue I have is the removal. With the healed microdermals, a small incision is needed to lift the “heel” of the jewelry out of the tissue. I’ve been using #11 scalpel to make this relief cut, but I’ve also heard of some practitioners using the side of a piercing needle. The other problem with the Industrial Strength microdermals is the rise on the base — all of which come in 3/32”, which I found a bit long for facial work. |
JOHN |
I’d like to be able to get the rise in a slightly longer length. I think in some areas an 1/8” rise is a better choice — being able to choose between the two would be great. |
WIZZER |
The prototypes I’m using now (made by IME of Integrity Body Jewelry) are available with as small as 3/64” rises, and in sizes ranging from 14 gauge to 10 gauge which work really well. This design also eliminates that “heel” which is found on the Industrial Strength microdermals and provides for a smoother insertion with a less invasive removal if removal is needed. |
IME |
I personally think that there is very little in the world that couldn’t use some refinement. Microdermals are no exception — just about everything can be improved on. |
JLO |
I am very happy with the Industrial Strength design — it’s certainly working well. I think Integrity’s design will probably work better in certain areas. IME is prototyping them, so we’ll have to wait and see. |
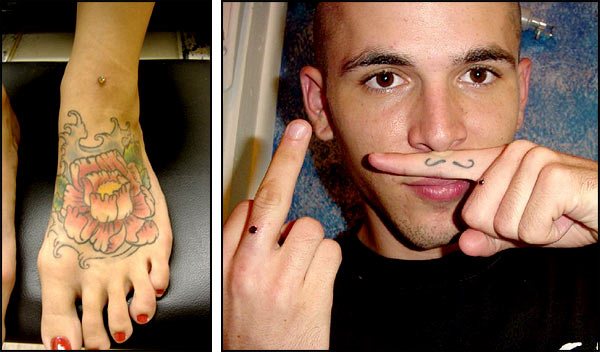
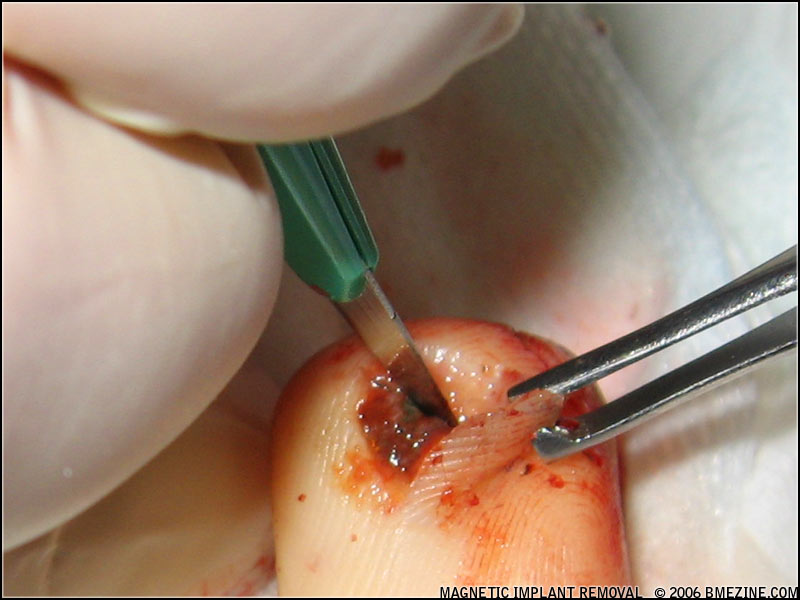
LEFT: FOOT BY DIDIER, RIGHT: FINGERS BY KEYLAN LEVINE (IAM:XKEYX)
| |
Do you think this has the potential to become a common or popular procedure? |
|
JLO |
Oh yes, I foresee them being as popular as nostril piercings at least. |
BRYAN |
They look awesome — I can see them being very popular! But I don’t feel that piercers should offer them to every customer that walks in the door — I don’t think the average customer is ready for something like this. |
DIDIER |
We’ve been trying to take our time working with these to assure they will be safe and effective for our industry. Things are just going so well with these that I see them being mainstream — even more than the surface bar. I see it staying as part of our list of standard procedures. |
IME |
I think so, for sure. It looks good on paper so far, but, it is a new thing — it’s going to take some time to see if they hold up. Personally I am very sceptical-slash-excited — as a piercer I’m just always making sure that what I’m doing is 100%, and a large part of that is the longevity of the end result. |
STEVE |
Microdermals definitely have the potential to become a popular procedure. I see more and more every day, but as their popularity rises I do fear low quality companies will start manufacturing shoddy representations of them without considerations for their usage. This has happened with virtually every type of jewelry so far, so I cannot imagine microdermals being exempt from it. Hand in hand, as they become more popular there will be a demand for low-cost procedures that might contribute to inexperienced — or uncaring — artists attempting them. Again, this has been true with virtually every new procedure we’ve seen. It seems inevitable, so I would urge everyone to make sure they feel comfortable and informed before allowing an artist to work on them — as you should with any procedure. |
PAT |
Yes, as you can clearly see, it will be popular. A week and a half from its debut at APP to a handful of people, Industrial Strength knocked off my design purely for the money and profit involved — they made insignificant changes, but, still, it was based on my original design. I was trying to test these out in a controlled fashion, put several out, get feedback, refine the design, do another test, and see if there are any issues with healing… But then Industrial Strength took this and ran straight into production, offering them to the masses, with no research, no development, and no testing. Because of this, several piercers are installing microdermals on a daily basis, making them commonplace, just like navel piercings. I guess time will tell on this.
…but, yes, these will be the “next big thing,” if they already aren’t already.
|
JOHN |
Commonplace, yeah, sure… popular, eh, I don’t know… It’s not going to be the next navel or nostril, but it may be the next surface piercing! |
| |
Anything else you’d like to add? |
|
DIDIER |
This is the first new anything to come along for piercing in a long while. More information will be available soon. I’ve been ask to sit on a panel on Anchoring for APP 2007, and look for a class through Professional Piercing Systems as well. |
JOHN |
I just want to thank Pat and JD for pushing boundaries and working on this design. |
IME |
Pat Pruitt of Custom Steel was the first person to start making these things and I feel that he has received very little credit this year. We as a community of jewelry makers in my opinion come up with all kinds of different things to make, and rarely do we get things like patents, seemingly leaving it to the “goodwill” of the rest of the community to not steal our designs — or start making something that is so similar to the original design that it looks like nothing but theft. |
PAT |
Aside from my personal soreness with a Custom Steel original being knocked off in record time, I think a word of warning should be sent out. That would be the long term applications of installing microdermals. Let’s not fool ourselves… this is an implant!!! This is not a piece of jewelry. I feel that removal down the road is still an unknown, and with the ease of insertion any Joe Hack piercer can install these… but removal on the other hand will require some skill. |

Shannon Larratt
BME.com
|




































































































































































{kind=link}