
|
“Nothing is legal with body hacking — so what!?! Why should we respect laws made by people who still believe that man should be like god made him? Why should we respect laws made by people who want to take the control of our destiny?”
– Lukas Zpira
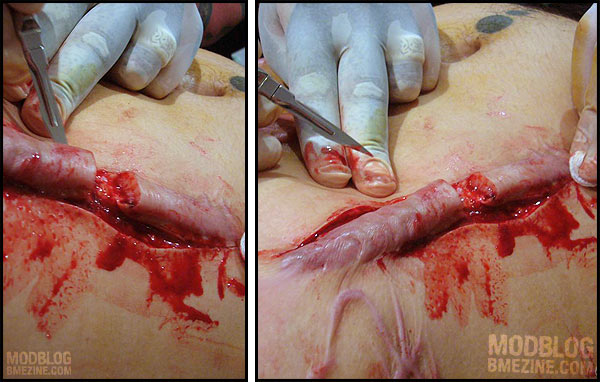
In a recent ModBlog entry I featured someone who’d had a skin removal scar done, which then keloided out of control, constricting his chest and negatively affecting mobility. Instead of going to a doctor or attempting non-surgical options, he chose to have two very experienced body modification practitioners cut off the keloids and stitch him back together (as seen in our scar repair gallery). From a risk point of view the procedure was arguably no more dangerous (perhaps even less, because of the wound closure) than a larger scarification project, let alone implants, tongue splitting, transscrotal piercings, and other common heavy modifications. To ensure healing went went, the practitioners stayed with the client (who was a practitioner himself) for a week afterwards, monitoring the process, and making sure he had full aftercare and treatment. As I write this the procedure is a success and the client is very happy with the results.
However, the two artists found themselves faced with enormous criticism accusing them of having irresponsibly “crossed the line” into medical territory, thereby endangering the client needlessly and putting others in the industry at risk should there be a legal snap-back if anything went wrong — which to me seems about as valid as telling gay men they can’t hold hands in public because it’ll freak out the heterosexuals, causing them to vote against gay marriage. Even though the reaction was likely a bit knee-jerk because the photos were quite graphic, there is some truth to the suggestion that the procedure may have been legally “medical” in nature because scar treatment is something doctors do and consider their territory. So even though in terms of difficulty or risk the procedure was less than almost all surgeries, it could have still caused a legal problem.
Depending on the nation it was done in, a wide range of charges could have been (and still could be) laid, including variations on practising medicine without a license and assault charges. Had the procedure been erotic in nature (subincision or castration for example), additional charges could be laid against media and websites posting photos and discussion of the procedure, including obscenity charges and record-keeping charges (for example, an American site has the legal obligation to share full identification information on the people in all photos of this type with the US government — thus BME is hosted outside of the US).
This all raises an interesting political question — why can’t I ask anyone to perform a “medical” procedure on me? Sure, I might be better off if I went to a doctor. But is it right to force me to go to a doctor? Do I not have the right to make the “wrong” decision? If not, why is it not my choice? It’s not as if I’m asking for the right to drunk drive or some other “wrong” decision that’s going to hurt others — I am asking only for the right of self-determination.
All human rights emerge from the belief that ultimately an individual has the right to choose their own destiny, and as such, all human rights and freedoms are built on the statement that we own ourselves. However, this runs contrary to the legal answer to the question I posed, because I can’t ask just anyone to do the procedure — I can only ask those who are approved by the government, and they usually have the legal obligation to refuse me if the procedure is in any way atypical.
“When there’s another person, if it’s a medical professional, you’re asking someone who is following the rules of the land to do something which, if it’s brand-new, has to be authorized by committee after committee after committee after committee and whatnot so he doesn’t get charged with manslaughter or assault and doesn’t lose his license.”
– Dr. Robert H. Stubbs, MD FRCSC FACS
So if I ask a doctor to do an atypical procedure, they are legally obligated to refuse (unless they’re willing to spend years justifying your case to their superiors). If I ask a friend to do it, they face a variety of criminal charges if they do it. If I do it myself, I risk medical imprisonment (psychiatric commitment, a process by which I can be permanently stripped of all my rights, and medicated against my consent to the point where I can’t defend myself). And if I do somehow get it done, and decide to talk about it publicly, I (or the hosting website that publishes my story and pictures) can be criminally charged for doing so. I think it should be very clear that there are broad limits as to our ownership of our own bodies, with the government determining what we are permitted to do and have done, and by whom.
In this sense, heavy body modification is an active form of political resistance against a system which seeks to make us prisoners under the guise of “protecting” us. Perhaps you agree that most of the time the government is right. Perhaps you are even correct most of the time. But that puts you in a position to help guide people, not to force them to submit to your opinion when it comes to their decisions about themselves. Forcing people under threat of prosecution and imprisonment to make decisions that “they’re better off” making is a slippery slope. Instead of arguing as to where to draw the line in terms of how much freedom the government should “give” people, what we should be arguing about is whether the government even has the right to draw a line telling us how much of ourselves we control and how much they control.
Actually, I’m not even willing to even have the debate — it’s black and white as far as I’m concerned. You can’t be “mostly free”. Mostly free equates to slavery. I’d rather make mistakes as free individual than be successful as a slave (that said, my intention is to be successful as a free individual!). Tell me that’s nonsensical all you want, or that maybe big brother knows better, but I’ve made lots of good decisions, and lots of bad decisions, and I value them all as a part of my life experience. I own myself, and I don’t need to be protected from myself. When I need help from the government, I’m comfortable asking for it. I’m not comfortable having it forced on me.
There are already many laws in place to protect us from the actions of others. A person who claims to be a doctor or otherwise misleads customers about their background can be charged. A person who abuses minors or engages in predatory behaviour (sexually, financially, or otherwise) can be charged. Negligence charges and many others can be used in the case of problematic or abusive practitioners. As far as I’m concerned the only laws in the realm of “practising medicine without a license” should have to do with people pretending to be doctors in name. The specifics of the procedure are irrelevant.
But when it comes down to it, the statement is quite simple:
I own myself. I can leave myself as I am, or I can improve myself as I see fit, or I can even choose to destroy myself. It’s my decision, and my decision alone. Any law that tells me that I don’t own myself, and can’t dictate what is done to by body and by whom, is fundamentally wrong and by definition a tool of those who would enslave others. Worse yet, it belies a flawed foundation upon which true human rights cannot be built.
Until society concedes total individual self ownership, freedom and rights are but a smokescreen.

Shannon Larratt
BME.com

























{kind=link}